Yep, still here and no trouble staying busy! We’ve been hit by a tsunami of free on-line content and software sales. The good news — it’s free (or at a discount). The bad news — the amount of time required to download, install, activate and maybe, gasp, actually use some of these samples, plug-ins, etc.
The list of free stuff is astounding. The Loopmasters, Loopcloud, Plug-ins Boutique and Producer Tech conglomerate has been veru generous during the pandemic and the summer season. The first stay-in and create promotion distributed:
These plug-ins are really worth it and useful. I Heart NY does parallel compression, good for mastering among other uses. Vocal Splitter separates mono vocals into stereo (ye olde split, delay and detune trick). Smasher is an Urei 1176 compressor emulation dedicated to the British all-buttons-in sound. Sure, the plugs are somewhat single purpose, but they sound great and are simple to use. Frankly, with all of this free content (!), I don’t have time to dial things in. 🙂
Sweetwater ran a promotion with iZotope, giving away the Ozone Elements mastering suite. Between Ozone Elements and Neutron Elements, that’s half of the iZotope Elements suite for nada.
I need to mention my favorite score from the Christmas holiday season: Arturia’s EMT-140 Plate Reverb. I have a fondness for plate and Arturia put together a beautiful EMT-140 emulation.
If that’s not enough, shake in the Korg software sale including Korg Module Pro and discount Cubase updates from Steinberg.
Plugin Boutique had a sale on zplane deCoda. deCoda is like Yamaha’s Chord Tracker on steroids, building on zplane’s experience in spectral analysis. Sure, it’ll identify the measure, sections and chords. However, you can draw MIDI notes on top of a spectral plot and export the MIDI to a file. A great way to capture a melody line from a song. deCoda has a focus panel which restricts analysis and playback to a specific frequency band and area within the stereo field. I see many uses beyond chord extraction!
Check out this introductory deCoda video. zplane have a v1.1 update in beta testing now. The beta adds the ability to save the chord progression to a file — a must-have feature. In v1.0, you need to jot the chords down by hand.
Hey, hey. If you keep your eyes and ears open, you can save some serious cash. The plugs and stuff mentioned here are first-rate, not sleazy hacks. Nows all we need is a time machine to learn, experiment, and put everything to good use.
I installed the free version of Module when I assembled the Korg NTS-1, hoping that it would unlock a few extra instruments in Module. For some reason, nothing unlocked and I gave up. I really wanted to assess the five built-in engines before springing for Module Pro.
Well, shucks, sight to the blind. Last week, I cast my gaze across the studio, coming to rest on the MicroKorg XL. Duh! Why didn’t I reach for the MicroKorg to begin with? After wiring up, the MicroKorg unlocked the electric piano, organ, clav, and string engines. Only one patch each, but certainly enough to get a good taste.
Needless to say, the five engines are pretty darned good. I sprang for Korg Module Pro and the Module Performance Expansion pack. The Module Performance Expansion pack adds more voices, MIDI CC learn and the ability to split and layer.
The ability to layer is very handy as I always find Korg’s acoustic instruments to be a little bit raw on their own. Sure, effects help to dress up the voices, but a soft pad adds warmth to strings and so forth. Orchestration 101.
MIDI CC learn is a bit of a necessity, I discovered. Unexpanded Module Pro responds to specific MIDI CC messages. For example, CC#100 controls organ rotary speaker speed, a rather essential element. To my chagrin, I discovered that the Yamaha MODX, which I am using as a controller, does not send CC message higher than CC#95! What the what? MIDI learn allows you to assign a controller to rotary speaker speed or other Module parameter of interest. [Check the update below for the correct solution!]
I connected the Yamaha MODX to the iPad via Apple Camera Connection Kit and an ancient IK Multimedia iRig 5-pin MIDI interface. Why 5-pin? That’s the other gotcha. I initially connected the MODX to the iPad via USB. Module receive the MIDI OK, but somehow the outgoing audio stream was lost with no signal at the 3.5mm headphone output. [See the update!]
I may look for a different audio/MIDI interface solution as I hate using the 3.5mm headphone jack. It’s not mechanically robust and it’s all too easy to get ear-itating scratchy audio. I don’t want to spend a lot of money and don’t want any solution involving powered hubs and such. I might give the Alesis Control Hub a try or maybe Korg’s own plugKEY. The Control Hub is a legacy product and availability is spotty. The plugKEY is a little more expansive, but is purpose-built for iPad software instruments and is Lightning-only. The Control Hub is USB-B class-compliant.
My only remaining nit is also one of my pet peeves. Software vendors should be forthcoming and specific about voices (patches) available at verious tiers. In the case of Kork Module, the free version has only one unlocked engine — acoustic piano and one patch:
Acoustic Piano Natural Grand
When the free version is connected to a Korg synth like the MicroKorg, you get five unlocked engines, one patch per engine:
Acoustic Piano Natural Grand Electric Piano Natural Tine EP Organ Simple Organ Clav Clav CA Strings/Choir Strings
The engine beneath Strings/Choir is really a sample-playback engine and it’s not limited to strings!
Korg Module Pro unlocks many additional patches for the five engines:
Acoustic Piano Natural Grand Bright Grand Dark Grand Heavy Touch Grand Light Touch Grand Damper Reverb Grand Cinema Piano Mono Attack Comp Piano Upright Piano Radio Piano Honky Tonk Flange Piano Electric Grand Chorus E.Grand AOR E.Grand Ac+El Piano Pad Piano Spacy Piano Strings Piano 1 Strings Piano 2 Choir Piano Twinkle Piano Stack Piano Electric Piano Natural Tine EP Hard Tine EP Soft Tine EP Tremolo EP Phaser EP Chorus EP Boomy Vibe EP Auto Wah EP Deep Mod EP Distortion EP Hybrid EP Dark Sine EP Digital EP Synthetic EP Pad Tine EP Strings Tine EP Organ Simple Organ Dark Organ Soul Organ Jazz Organ Memphis Organ Gospel Organ Clean Organ Bright Organ Drive Organ 1 Drive Organ 2 Full Organ 1 Full Organ 2 Perc Organ 1 Perc Organ 2 Perc Organ 3 Perc Organ 4 Vox Organ 1 Vox Organ 2 Clav Clav CA Clav CB Clav DA Clav DB Wah Clav Phaser Clav Distortion Clav Mute Clav Psychedelic Clav Clav Guitar Sample-playback Strings Slow Strings Strings Pad Analog Strings Phase Strings Flange Pad Choir Pad Vocoder Pad Brass Ens Octave Brass Funky Sfz Brass Hybrid Brass Analog Brass Soft Horn Warm Pad Saw Pad Ambient Pad Bell Pad Saw Wave Chiptune Wave Synth Stab Unison Synth Saw Synth Soft Synth Rez Comp Rez Square Synth Clav Saw Pluck Square Pop Detune Sine Digital Bell Ring Bell
The electric piano is quite nice; the patches provide a wide range of Rhodes tone. The rotary organ patches cover a useful range, too, including a pair of VOX combo organ sounds. The clav is up-to-snuff and the patches cover the usual favorites. The sample-playback sounds are strong on ensemble voices, not so much lead tones or solo instruments.
The Module Performance Expansion pack rounds out the sample-playback sound set with guitars, bass, solo instruments, etc.
Sample-playback Violin Cello Pizzicato Chamber Strings Strings Ensemble Tremolo Strings Romantique Strings Synth Strings A Capella Pad Bubble Choir Solo Trumpet Band Brass Fanfare Horn Ensemble Synth Horn Solo Flute Vibrato Flute Pan Flute Alto Saxophone Tenor Saxophone Wind Ensemble Chamber Orchestra Unison Stab Mono Dark Lead Mono Synth Lead Detune Saw Lead Octave Lead Talking Lead Analog Piano Synth Pad Piano Velocity Synth Synth Pad Dark Pad Snow Pad Aurora Pad Artificial Effect Filter Motion Air Organ Vibra-phone Glockenspiel Celesta Steel Drum Tubular Bell Mysterious Bell Vibrato Glass Bell Bell Tower Pad Foggy Hills Ac. Guitar Nylon Guitar Electric Guitar Guitar Dist. Harp Sitar Ac. Bass Walking Jazz Bass Fretless Bass Finger Bass Mute Pick Bass Slap Bass Fat Pulse Bass Filter Bass
All of these sounds can be used as layer elements, too. That’s a lot of detail, but it should give you a better sense of the product feature tiers.
Update
After spending more time with Korg Module Pro, I’m happy. The sounds are first rate without much filler or junk. Some of the sounds are inspiring.
Further experiments…
I connected the Yamaha SHS-500 keytar to Korg Module Pro over Bluetooth MIDI. Pairing was a breeze, I couldn’t discern any annoying latency at all. There are a few patches where I dialed up the effect level — par for the course. I can see the SHS-500 plus iPad/Module as a lightweight portable rig. Going wireless would be a real boon for the crazy small spaces that I play in.
I also gave MODX another shot as MIDI controller. Success! The digital audio stream is sent back to MODX on its USB class-compliant audio device. My initial mistake was a head-slapper. Pay attention to the MIDI and audio meters in Module’s upper left corner. At first, I saw MIDI activity and no outgoing audio level. Should have been a big clue. Check and set Module’s OUTPUT LEVEL knob and make sure it’s turned up. Doh!
I resolved the organ rotary speaker speed issue by reading the manual and noting the organ/damper pedal setting. Module receives CC#64 sustain. When the organ/damper pedal setting is “Rotary,” sustain toggles the rotary speaker speed — no MIDI CC learn is necessary.
That’s it! Korg Module Pro 50% off is money well spent.
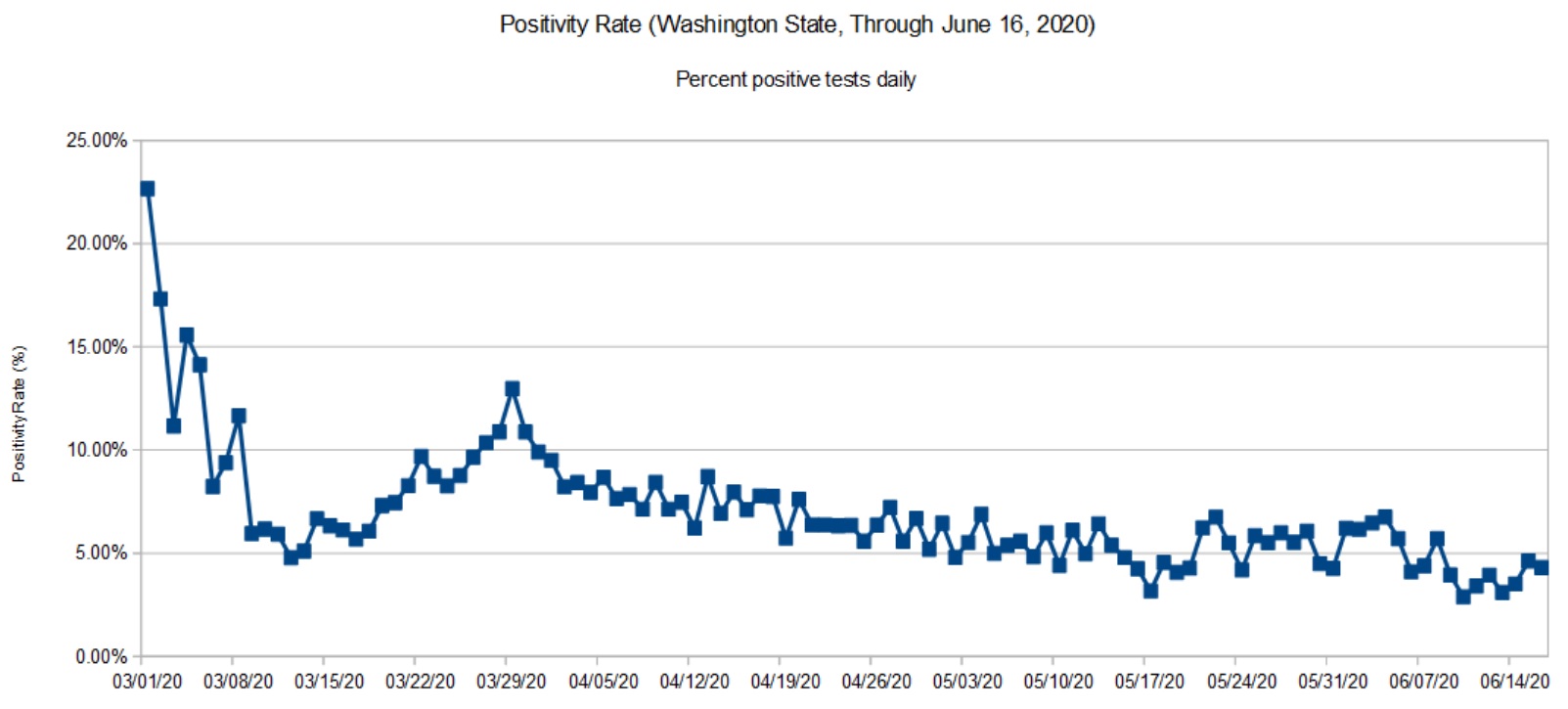
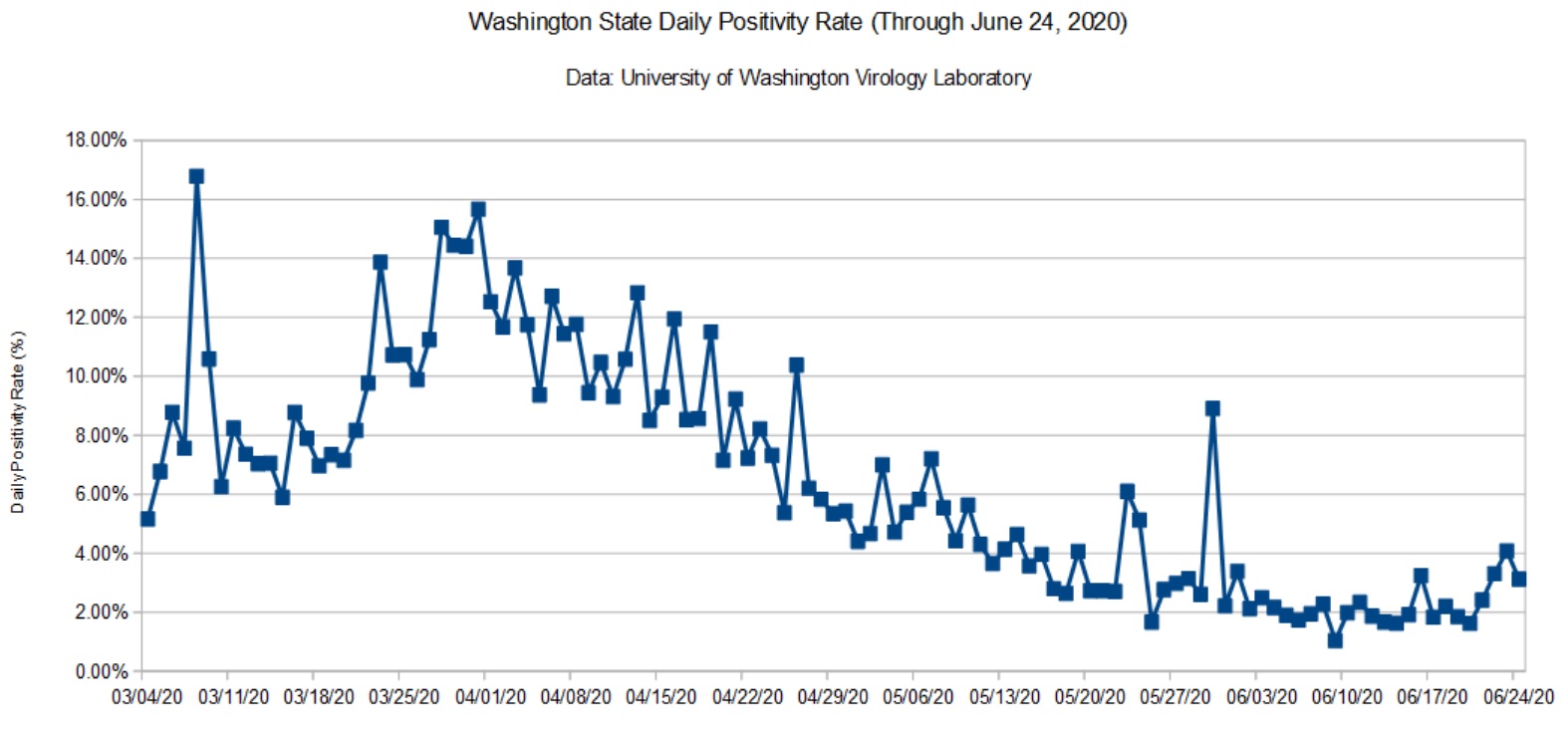
Here is my COVD-19 update taking us through June 24, 2020. Data are taken from the Washington State Department of Health (DOH) and the University of Washington Virology Lab (UW). The DOH data are complete through June 16, 2020 and that is what is shown here. [Click images to enlarge.]
Washington State Positivity Rate (DOH, June 16, 2020)Washington State Positivity Rate (UW, June 24, 2020)
We’re seeing a small uptick which is probably due to the BLM protests in Seattle (early June) and the worsening situation in Yakima County. My daily tracker indicates a roughly 5% positivity rate that is consistent with the charts above.
The recently announced NY/NJ/CT travel quarantine initially included Washington State. That really surprised me and sent me diving into the data. However, it appears that the NY/NJ/CT authorities reacted to a temporary “condition” in the data. Giving them the benefit of the doubt, the DOH did a massive update recently, taking seriology tests out of the daily testing statistics. I took a numerical tour of the hottest states recently and was appalled at the inconsistency and shortcomings in reporting. (CDC? Hello? Anybody home?) Confusion is somewhat understandable.
Several weeks ago, I decided to record the church tunes that I enjoy playing. It’s best to start with favorites, as most of you know how you come to detest a track after playing it over, and over, and over again during production. Energy quickly dissipates when micro-editing MIDI events or digital audio…
Before getting into production notes, here are links to the final tracks (all MP3). The goal was to crank out a new tune each week and send it to the folks in our music ministry. Some tunes are a little more polished than others. Please consider them “demo quality.”
Without going too far into the technical weeds, the primary sound source is Yamaha Genos™ and the primary vocalist is my spouse Fran. With the Mill Creek Chorale on hiatus — aren’t we all? — I was happy that she could contribute and have fun, too.
Production notes
So, how did all of this go down?
These demoes show off the Yamaha Genos as a sound source and production tool. I had two main subgoals:
Learn how to record a demo with Genos in either audio or MIDI format.
Learn how to mix down with Steinberg Cubase Artist and try out a few of the freebie plug-ins that I’ve collected.
By and large, Genos and Cubase were the main production tools although I back-slid into SONAR on a few occasions for MIDI editing. Old habits die hard. Workflow was not strictly linear from Genos to Cubase. In a few cases. MIDI and/or audio (stereo 16-bit 44,100 WAV) were slung back and forth between tools.
Yamaha Genos
Genos is the sound source with one big exception: drawbar organ. When you hear B-3, you’re hearing Yamaha MODX through an Electro-Harmonix Lester K. I wanted to hear Lester K in musical context. It sits in a song pretty well and has more guts than the Yamaha MODX Leslie simulator. By itself, though, Lester K has some high-end swirliness in the upper drawbars, but in a track, it seems to mesh. You be the judge.
Emphasis was on speed. Get the tracks down quickly and finish a song each week ASAP. The Beatles used to call this recording “on heat.” Even so, it’s amazing how modern technology will drag you into the dank chasm of production minutiae. Don’t you just love hearing the same three measures fifty times while tweaking and tweezing. Not.
All vocals were recorded directly to Genos using its microphone input. Full backing and raw vocal tracks were exported to Cubase via WAV. Everything was processed and mixed in Cubase. The final mix was exported from Cubase as WAV, and then trimmed and converted to MP3 using Sound Forge Audio Studio.
Our God Is Here This was the first demo in the series and the process doesn’t get any simpler than this. All was recorded into Genos Audio Multi Recording. Find a beat, turn it on, lay down the organ part. Unfortunately, I didn’t plan for the ending, which is quite ragged. The organ is Genos in this case (not MODX). Kinda plain, huh? The bass is an overdub.
Audio Multi Recording is a nicely done sound-on-sound recorder a la Les Paul, minus tape hiss. There are two stereo tracks: main and sub. You can record directly to either main or sub, and bounce (sub+main) to main. There are options for punch in and overdub. Audio Multi Recording provides WAV import and export, functionality which eventually got a true work-out.
Audio Multi Recording keeps digital audio in a persistent project. A project resides in the internal Genos 60GB user solid-state drive and is always ready. The project remembers audio and mix settings without requiring explicit save and load user operations. That makes for a clean workflow. Export is the way to get digital audio into a WAV file and it mixes the main and sub on the way to WAV. In order to export a solo vocal track from sub, one needs to dial down the main and then wait while Genos writes the WAV file in real time. I wish there was a simple, direct fast export to WAV supporting both main to WAV and sub to WAV.
In The Day Of The Lord I quickly realized that I do need to think ahead and assemble a basic skeleton on which I could build a tune. (Duh!) In this case, Toontrack EZDrummer provided the drum patterns which I pulled together in Cubase. Genos played the MIDI drum track while I recorded the flute as a melodic guide and layered in the bass and organ — all recorded as audio. We then did a few vocal takes to Genos. I transferred all of the Genos audio as WAV into Cubase for the final mix. Vocal processing typically was light: a little pitch correction, EQ, and maybe double tracking. A touch of reverb (Cubase Revelation) blends everything together here.
Stop By, Lord This tune makes use of the Genos rhythm accompaniment consisting of main patterns and one-bar fills. I recorded a basic guide track in MIDI using the “BigBandBallad” style as the drummer. This meant switching the main and fill patterns with my left hand while playing the melody with my right hand. I layered in the piano, bass and horns, discarding the guide melody along the way. I added the B-3 organ (MODX through Lester K) in an audio pass. Everything was recorded and produced on Genos since we didn’t record vocals.
Psalm 95 If Today “If Today” makes full use of the Genos arranger features. I played the basic accompaniment track using the “Sunny Reggae” style. Whoever built that style, it must have been a labor of love and it fits this song quite well. I vocoded my voice. Both the accompaniment and vocal tracks where exported to Cubase for final assembly and mix down. I had a lot of fun adding dub effects and tons of reverb, Long live King Tubby!
Rise Up With Him “Rise Up” was recorded to MIDI, again using the Genos rhythm accompaniment as the drummer. The electric piano went down first followed by the bass. The B-3 organ is MODX through Lester K. Backing and vocal audio were exported to Cubase for final mix down. Overall, a pretty simple demo to pull together.
O Sacred Head I recorded the MIDI for this tune a long time ago — in the early 2000s on a Roland XP-60. The guitar picking was carefully edited and assembled (years ago!) from Twiddly Bits. I imported the XP-60 MIDI into Cakewalk, choosing Genos voices and effects. The Genos result versus the original XP-60 is amazing. Fran encouraged me to leave it as an instrumental.
This Is The Day This psalm is long out-of-print. A few years agao, I transfered a scruffy copy of the piano score into Sibelius. So, to kickstart this tune, I exported MIDI from Sibelius, restructured the sections, and humanized the piano as much as possible. I tried to keep the accompaniment simple adding just bass and horns. Once again, the backing and vocal tracks were mixed in Cubase. This demo is a good example of Arturia’s Plate-140 reverb — a freebie that Arturia gave away during the Christmas holiday. I love it.
Lead Me, Lord Another simple turn-on-the-beat-box, sound-on-sound production. Everything was recorded to Genos with the backing and vocal tracks exported to Cubase. (Another example of Plate-140, BTW.) The vocal harmony was generated by a TC Helicon Play Electric added in real time. Recording and production was dirt simple although it took a while to get the TC Helicon configured.
Alleluia! Love Is Alive This was the penultimate demo in the series. The basic track is a stripped down Genos “6-8PopBallad” style. Yamaha tends to over-orchestrate styles, so I kept drum, bass and guitars, tossing the rest. Instead of playing the basic track, I created the accompaniment using chord step-record. This MIDI Multi Recording feature lets a musician enter chords and sections from a lead sheet, quickly creating the song skeleton. You can even try different styles if you haven’t chosen one already. Once the skeleton is set, you expand the chord track into MIDI events, thereby obtaining the full backing track in a Standard MIDI File (SMF).
I added the Celtic violin by playing it into a free MIDI track. Using Sonar, I tweaked the tempo in the full MIDI song in order to add energy as the song progressively builds to the end. Finally, with the MIDI finished, I froze the backing tracking to WAV audio. The backing and vocal tracks were mixed down in Cubase with a little automation here and there to add vocal depth and double tracking.
Conclusions?
The preceding discussion is already a lot to absorb and to process. I’ll take a step back in a future post and try to summarize. All the best to ya.
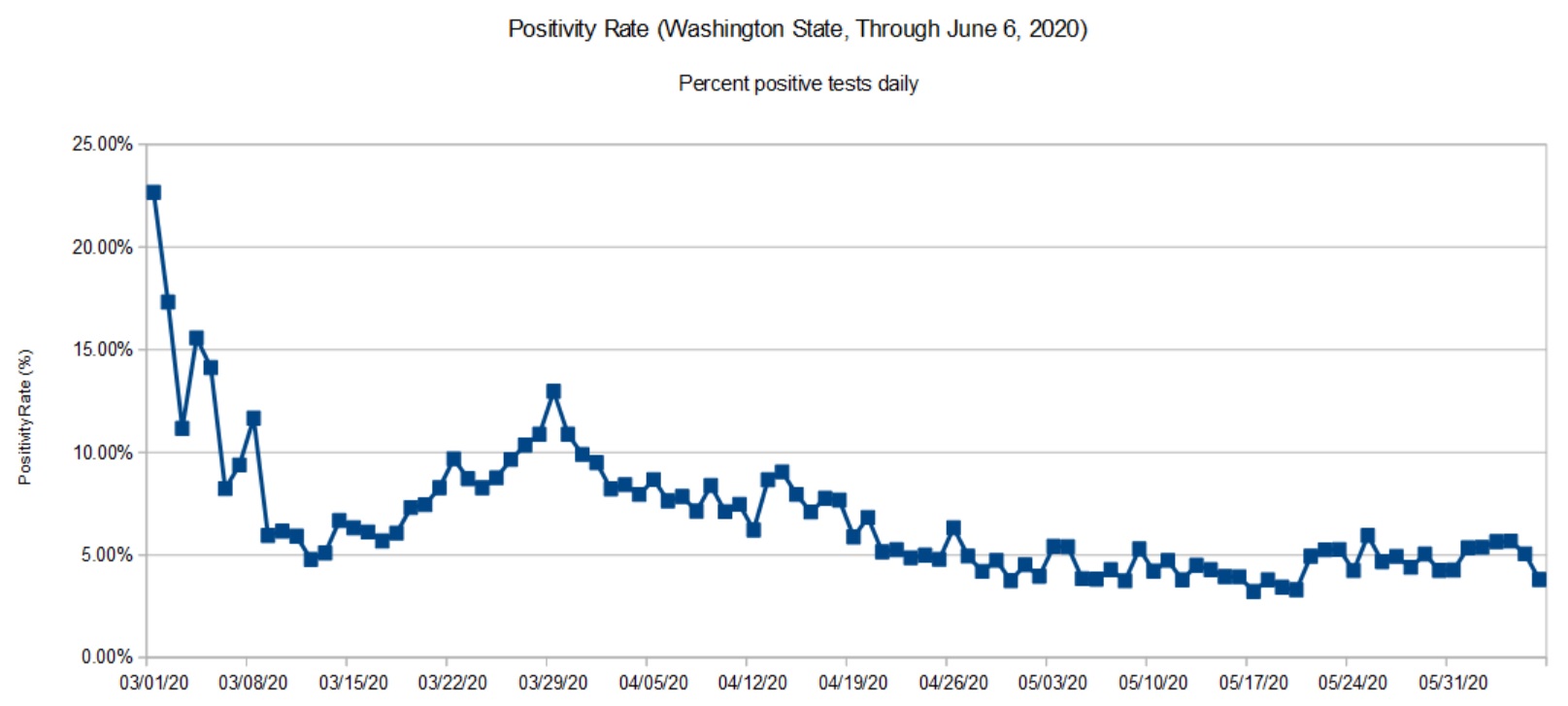
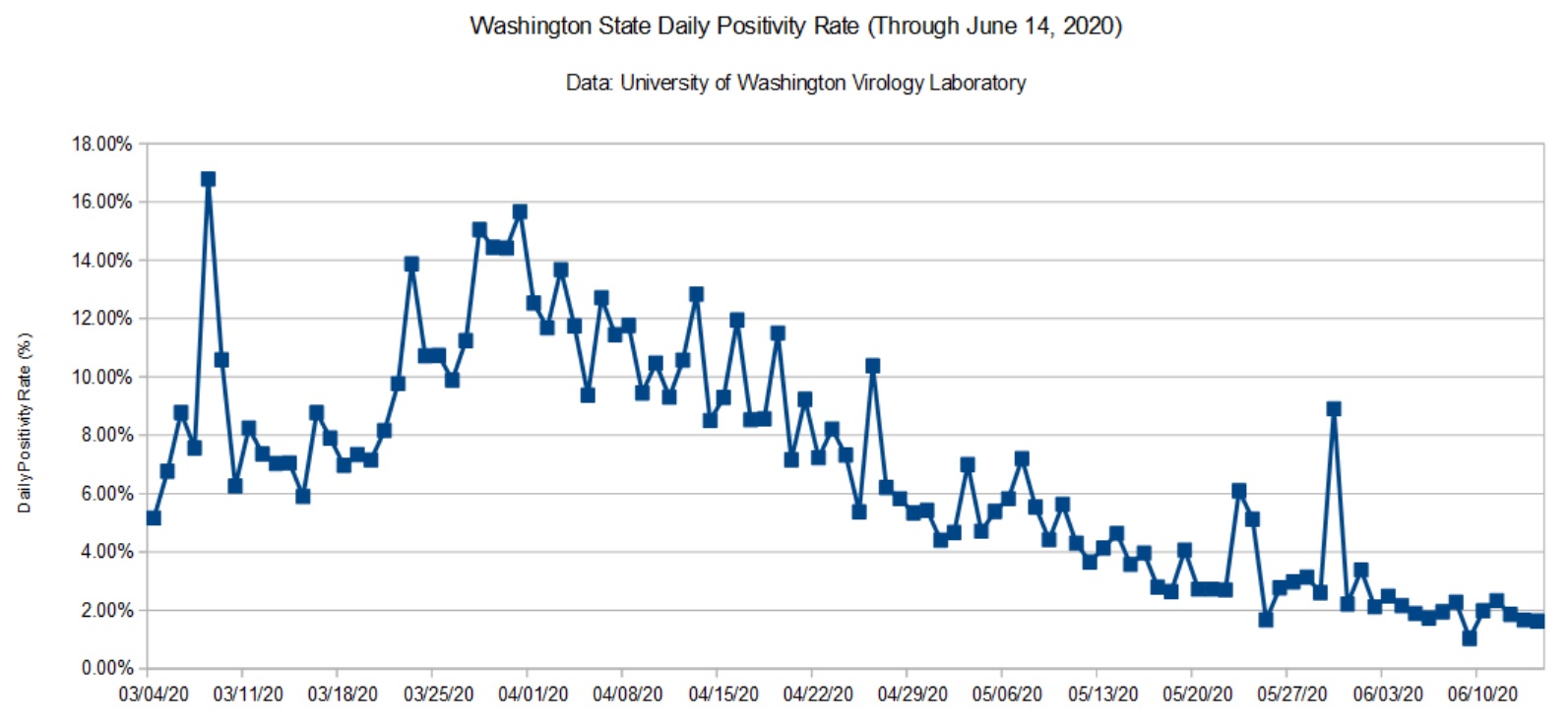
Here is my latest update for the COVID-19 positivity rate in Washington State. The Department of Health (DOH) data are relatively complete through June 6, 2020 and the University of Washington Virology Lab (UW) data are complete through June 14. [Click images to enlarge.]
Washington State daily positivity rate (DOH, June 6, 2020)Washington State daily positivity rate (UW, June 14, 2020)
The DOH rate was roughly 5% at the beginning of June. The UW rate is slightly lower, around 3%. The UW rate and my daily tracker do not indicate a rise due to the recent protests in Seattle (King County). I hope the rate remains low or declines further.
Washington State has added considerable test capacity in recent days. During most of May, the State performed about 4,000 to 5,000 tests per day. Now, the State is performing about 10,000 tests per day. The UW dashboard shows a big increase in their test capacity.
Although the situation in King and Snohomish Counties has improved, a few counties in eastern Washington — most notably, Yakima County — are deteriorating.
Mobility
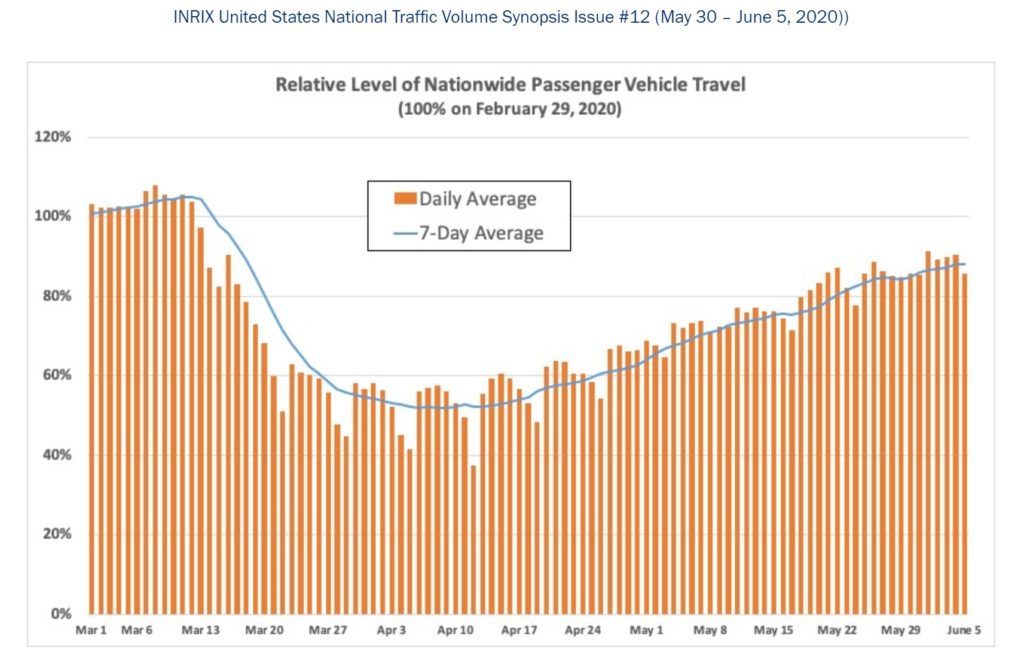
INRIX is a traffic management company which bases its analysis on road sensors and vehicle data. As a public service, INRIX posts an analysis for nationwide vehicle travel data to assist the COVID-19 fight. I recommend visiting the INRIX COVID-19 pages. You will find several informative tables like the one below, plus a national heat map depicting the change in travel at a few snapshot dates (April 11, May 24, May 29).
Traffic volume hit a lull in early April and has been steadily increasing in many parts of the United States. Travel is still lower in certain urban centers, especially those which were hardest hit by COVID-19. Rural travel has come roaring back.
INRIX has heat maps for key urban centers. So, if you want to see how your city is doing, be sure to visit their pages. The Seattle area heat map shows higher traffic, which is consistent with my personal (anecdotal) observations.
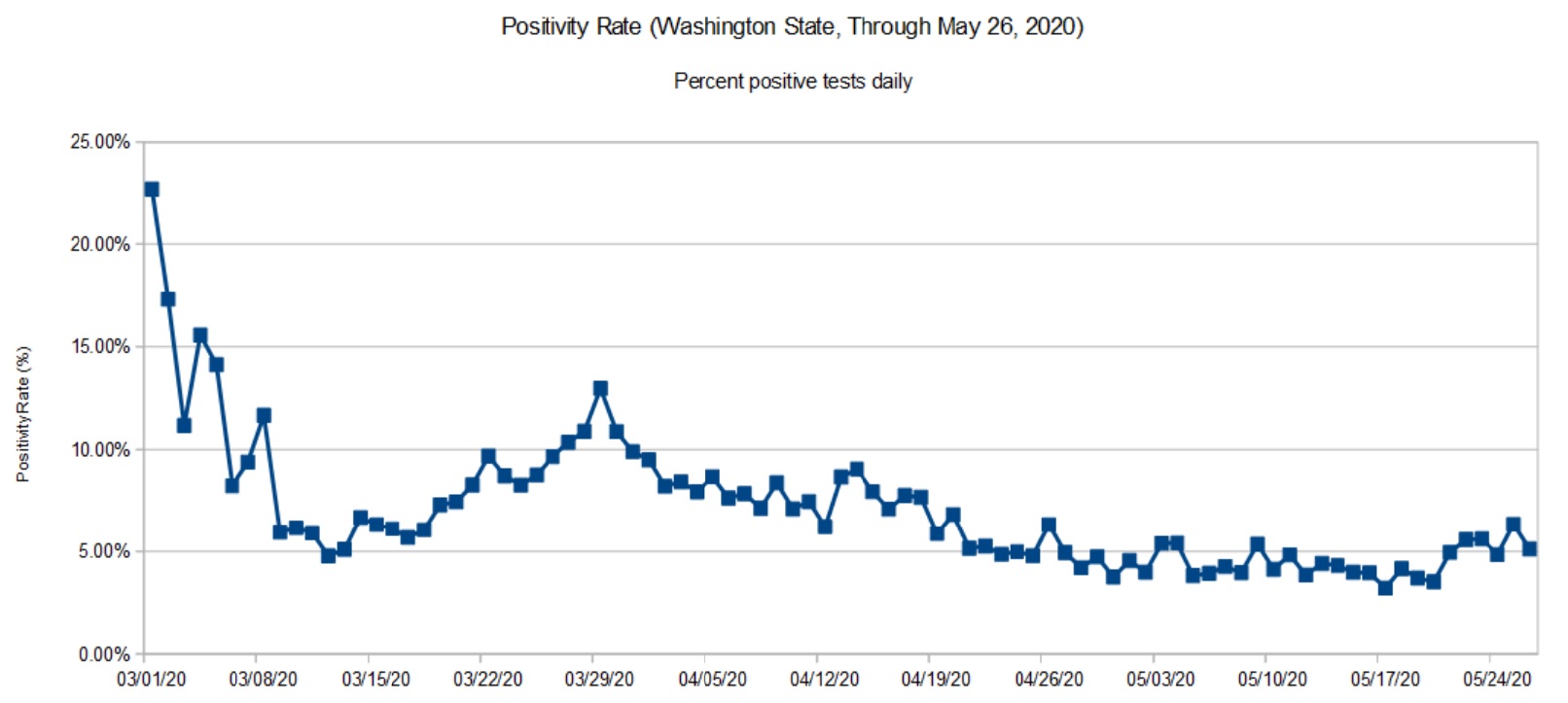
Washington State Daily Positivity Rate (DOH, May 26, 2020)
The DOH positivity has taken a definite upswing during the last week. Folks are getting antsy and highway traffic is noticeably heavier. The morning traffic report is back to yellow and red trouble spots on the local highways. Mobility has definitely increased as we will probably see in the next report from the Institute for Disease Modeling.
It will be 10 to 14 days before we see the effect of protests in the Seattle area. Large gatherings of people are definitely spreader events.
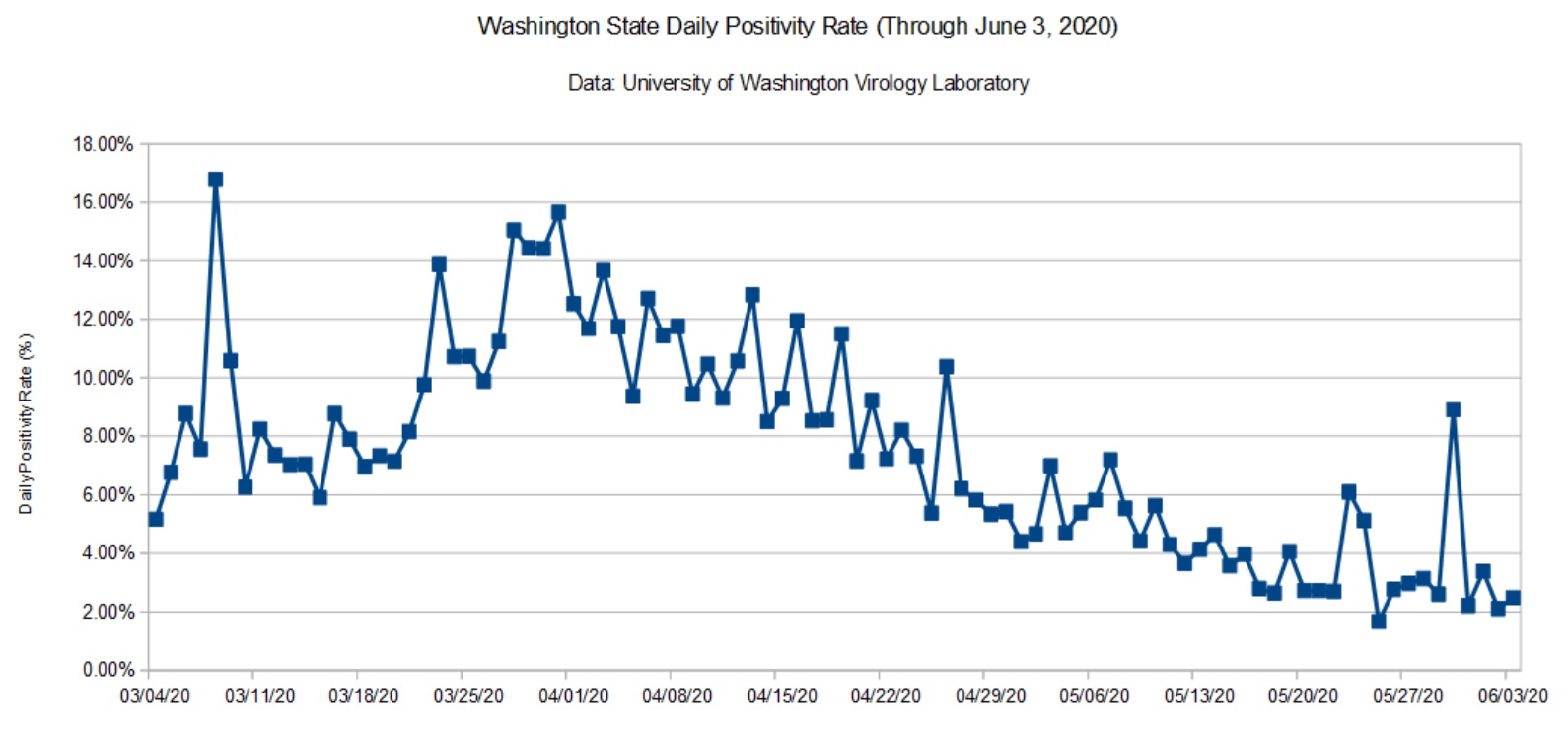
Washington State Daily Positivity Rate (UW, June 3, 2020)
The data from UW had a localized bump. This may be the result of contact tracing within a cluster. I wish the UW site was a little more informative, but interpretation is really DOH’s job.
I still see and hear local media reporting observations like “The number of cases dropped dramatically yesterday.” Raw case counts are relatively meaningless unless the number of tests are taken into account. That’s why I’m tracking the daily positivity rate — the percentage of positive test results for each day.
Here’s an example to show what I mean. Testing (and reporting) dips over the weekend. The number of weekend (Saturday and Sunday) tests is typically less than half of weekday tests. Here are the mostly values reported in the media
The first three columns are the cumulative metrics published by DOH. The last three columns are the number of positive tests, tests performed and positivity rate for each day. The date is the reporting date, so June 1 (Monday) covers the preceding Sunday.
Please note how fewer tests are performed on Sunday than Monday. Sure, the number of raw positive cases on Sunday is dramatically lower Monday. However, the positivity rate is higher for Sunday is actually higher. Yep, the local news station was touting the Sunday number! This is fundamental numeracy, people.
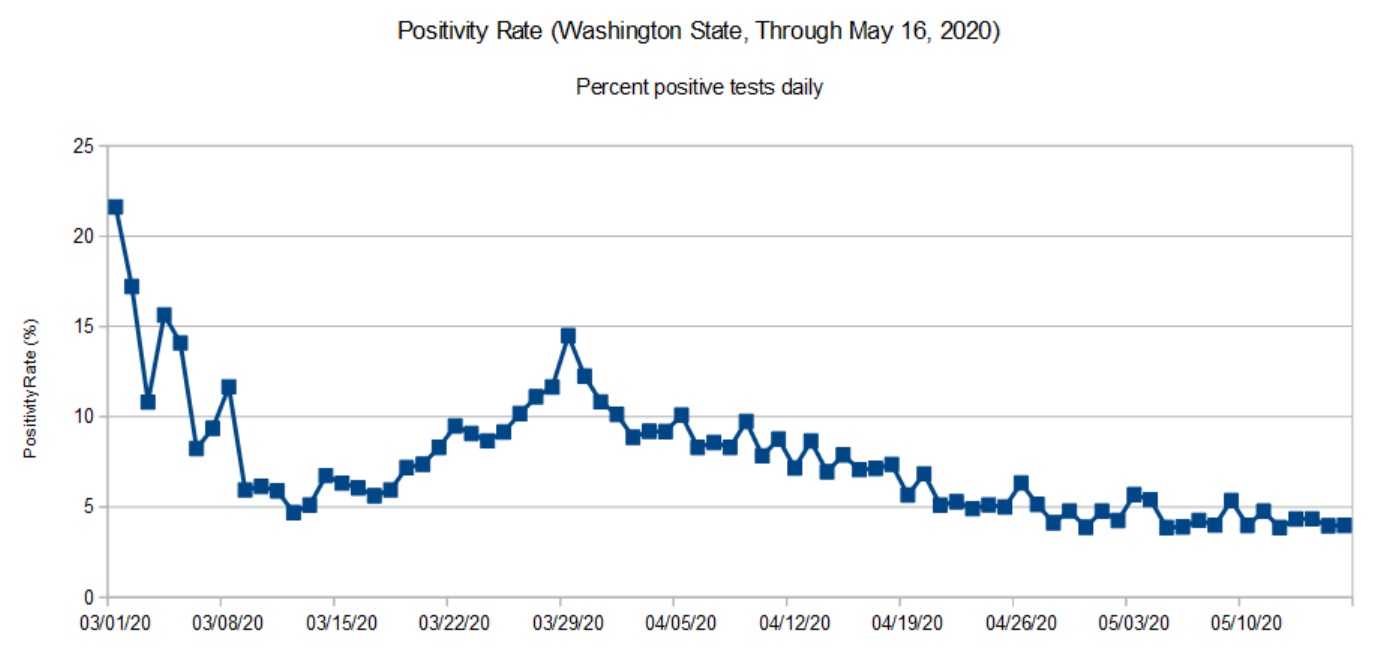
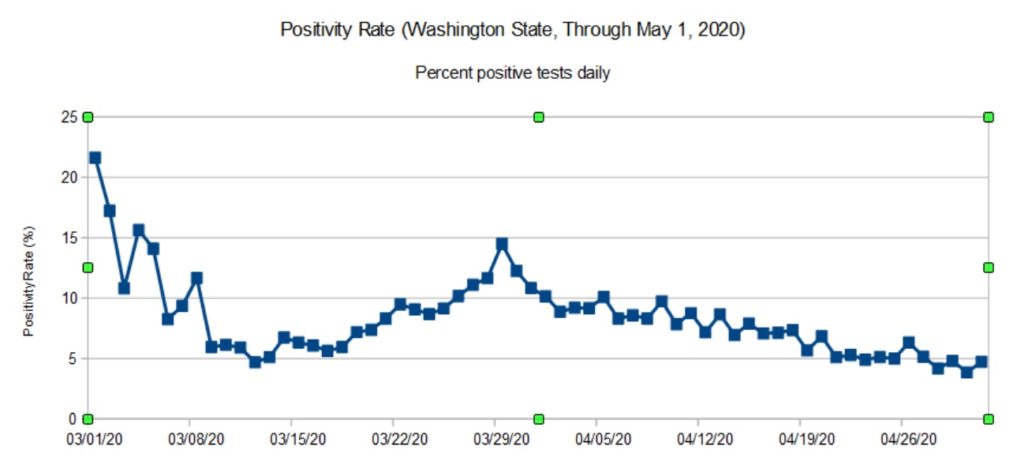
As noted in previous posts, data from the Washington State Department of Health (DOH) lags a little bit as reports arrive from county health departments. So, the DOH chart (below) covers the period up to May 16 (about ten days ago at the time of this writing).
Washington State daily positivity rate (DOH, May 16, 2020)
The trend in the DOH daily positivity rate (percent positive tests per day) is decidedly downward. It’s worth noting, however, how fast a community can move up the curve than down. The difference between the upward slope and downward slope should make people cautious — we don’t want to be on the wrong side of the curve again. It’s better to knock the disease to its knees and keep it there than to suffer a series of waves, even small waves.
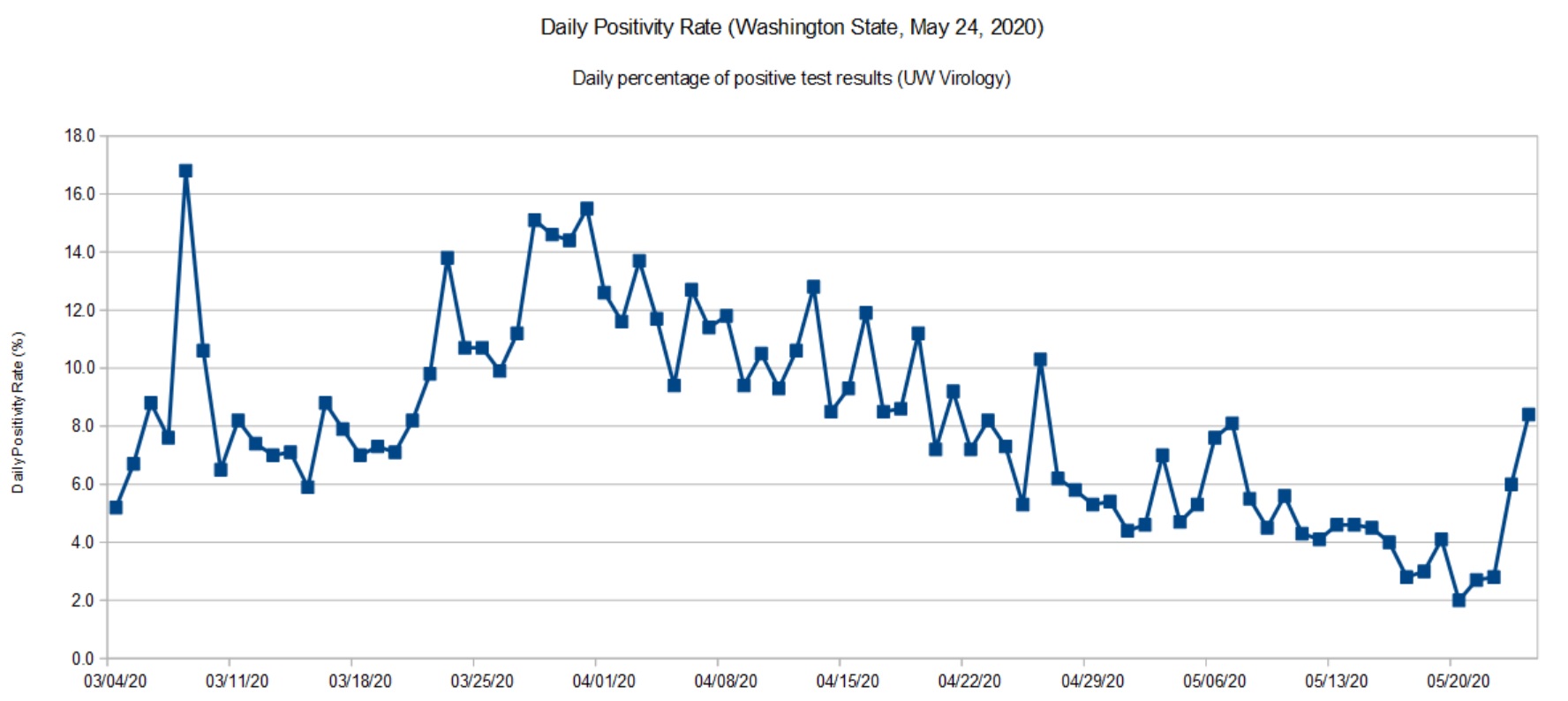
Washington State daily positivity rate (UW, May 24, 2020)
I don’t see a similar up-turn in the latest daily stats from the DOH, so I’m quite curious as to the cause for a higher positivity rate in UW’s most recent data. Did the lab test more samples from a COVID-19 cluster under investigation? Are there quality issues with the samples or test materials? I hope that they are looking into these questions.
I recommend reading this excellent report from the Imperial College COVID-19 Response Team: H Juliette Unwin, Swapnil Mishra, Valerie C Bradley et al. State-level tracking of COVID-19 in the United States (21-05-2020), doi: https://doi.org/10.25561/79231
The report provides a timely analysis and summary of COVID-19 in the United States, including an estimate of the effective transmission rate (Re) for each state. The report is licensed under a Creative Commons Attribution NonCommercial NoDerivatives 4.0 International License.
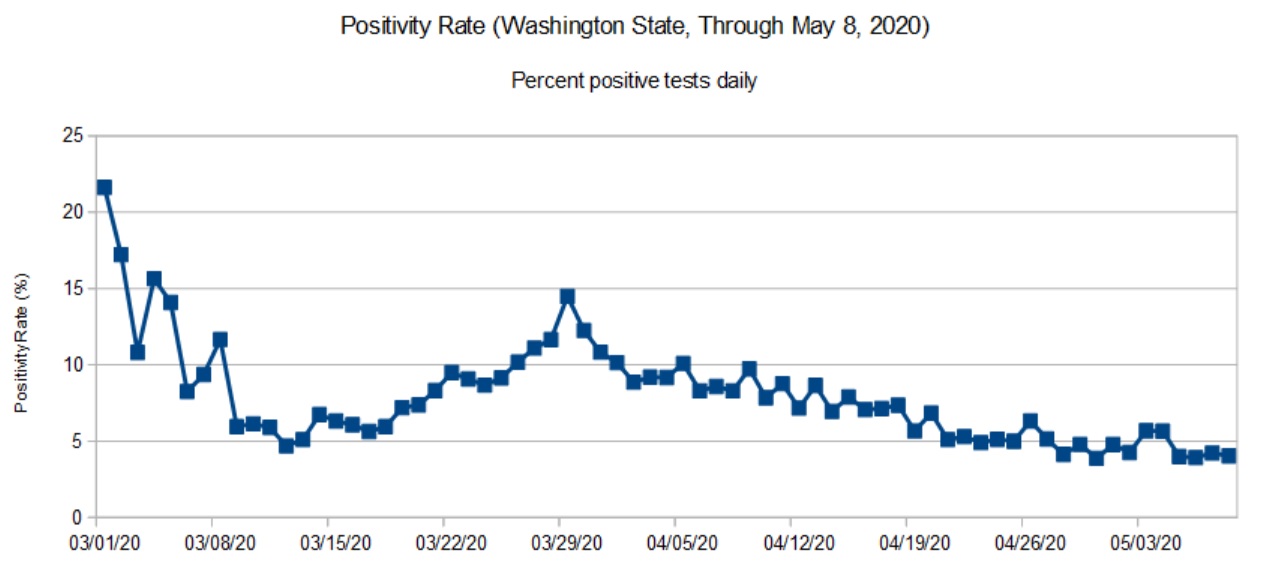
Daily positivity rate for Washington State (DOH, May 8, 2020)
The DOH reports (relatively) complete data through May 8. That’s why the title of this page refers to “May 8” even though I’m posting these charts on May 18.
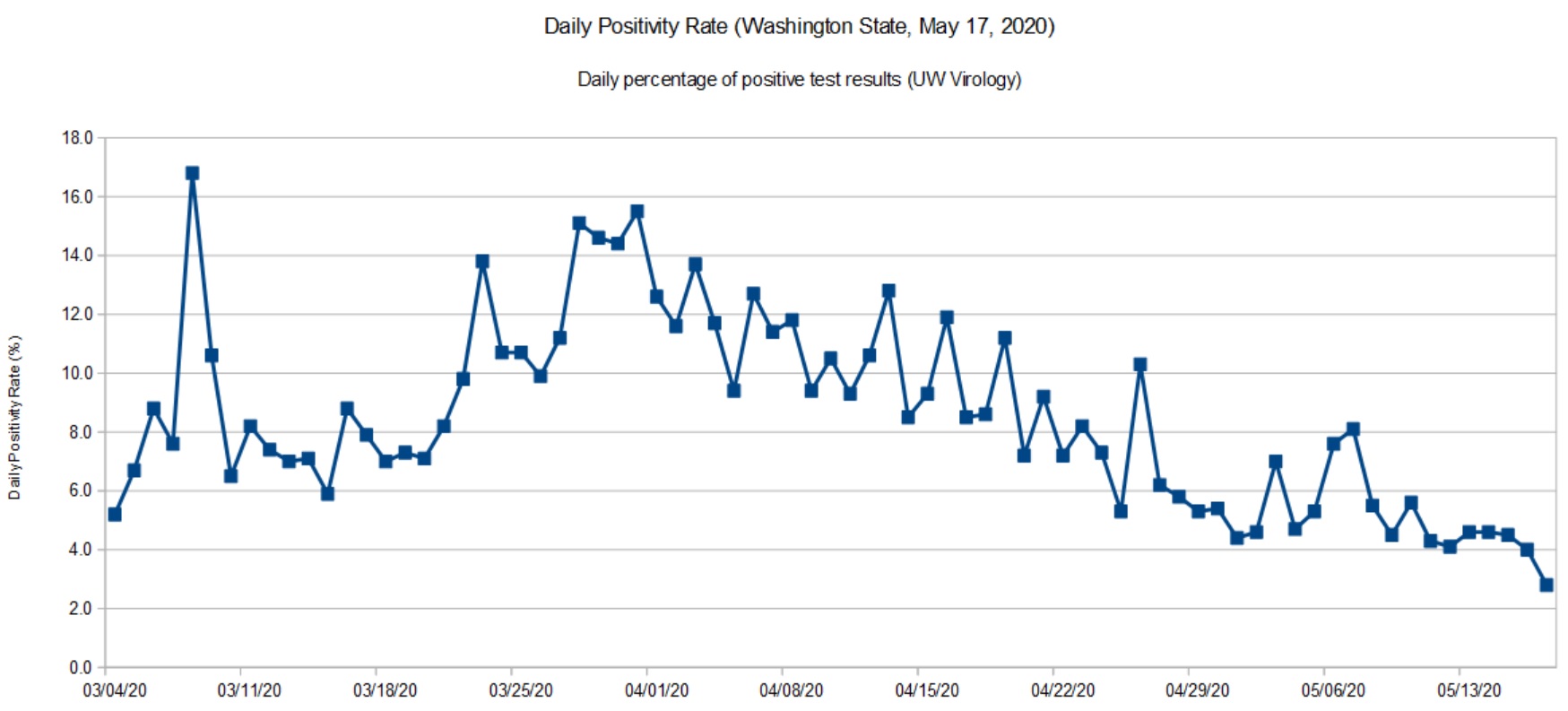
The UW Virology Laboratory performs a significant portion (about 40%) of the COVID-19 testing in Washington State. Approximately 90% of the tests performed by UW are for patients in Washington itself. [Click images to enlarge.]
Daily positivity rate for Washington (UW, May 17, 2020)
The UW data is current up to the present date (May 17, 2020). So, you may think about UW’s positivity rate as a glimpse at the past week before the DOH statistics roll out. Like the DOH trend, there was a slight up-tick at the end of April and beginning of May, which is now settling back down.
I’m quite happy to see the downward trend and that we are keeping the disease in check. We are going to the dentist tomorrow (!) and it will be interesting to see how they handle the situation.
The virus is still out there. The CDC MMWR should make everyone wonder about choir/music rehearsals and performance in the near- to medium-term future. We need to take this health threat seriously until people are vaccinated.
After making slow progress against COVID-19, Washington State lost a little ground during the last two weeks. We aren’t heading up the steep slope, but the unusually good weather has brought people out of isolation.
Here we see a more definite up-tick in recent days. As a state, we need to double-down on social distancing — it’s too soon to give up! I don’t think anyone really wants to go through another long lock-down. It’s better to quash COVID-19 and keep it down. Anything less delays economic recovery.
The Institute for Disease Modeling (IDM) estimates the effective reproductive number (Re) for King County, Washington. King County is the most populous county in Washington covering much of the Seattle metropolitan area. (Snohomish County fringes on the metro area, it’s main population center is Everett.)
IDM reports both a likely range for Re (95% confidence interval) and a best estimate for its value on a particular date. The table below summarizes their findings:
Date Lower Upper Best Est -------------- ----- ----- -------- March 25, 2020 0.30 1.20 0.73 April 4, 2020 0.55 1.33 0.94 April 15, 2020 0.28 1.00 0.64 April 27, 2020 0.47 1.32 0.89
IDM base their analysis on data from the Washington Department of Health and mobility (traffic) data. IDM’s best estimate of cumulative incidence through April 20 is 2.1%, meaning that 2.1% of the community has or has had COVID-19 as of April 20.
Worrisome, IDM hasn’t found Re to have dropped definitively below one for Eastern Washington. Although Western Washington has made progress, Eastern Washington is not improving. The number of new cases tracks Re. When Re increases, the number of new cases increases, too, lagging in time by the COVID-19 incubation period.
Please remember that we are shooting for an Re less than one, meaning that the spread of SARS-CoV-2 (the virus which causes COVID-19) is slow enough to prevent a rapid rise in new cases. Social distancing, contact tracing and isolation are all about keeping Re as far below one as possible.
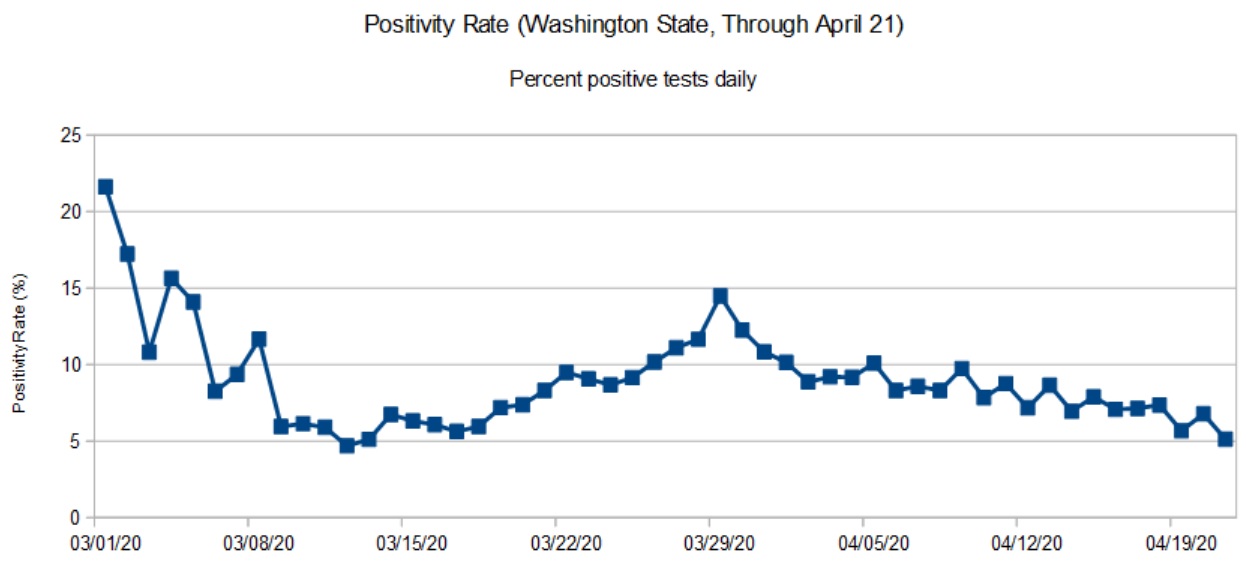
To kick things off, here are my latest graphs for the Washington State COVID-19 positivity rate. The positivity rate is the daily percentage of positive COVID-19 tests. Like the daily new case count, we’re hoping to see a downward trend over time as community mitigation (AKA “social distancing”) slows the effective infectiousness (REFF) of SARS-CoV-2.
Washington State daily positivity rate (DOH, April 21, 2020)
The first graph is based on data from the Washington State Department of Health (DOH). DOH aggregates data across the entire state. Data for most recent days are incomplete and I have not included partial results in the graph.
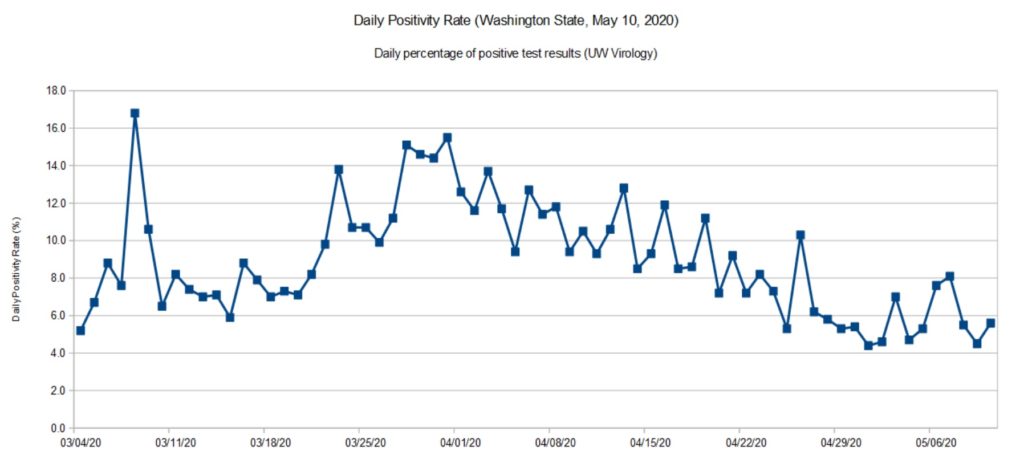
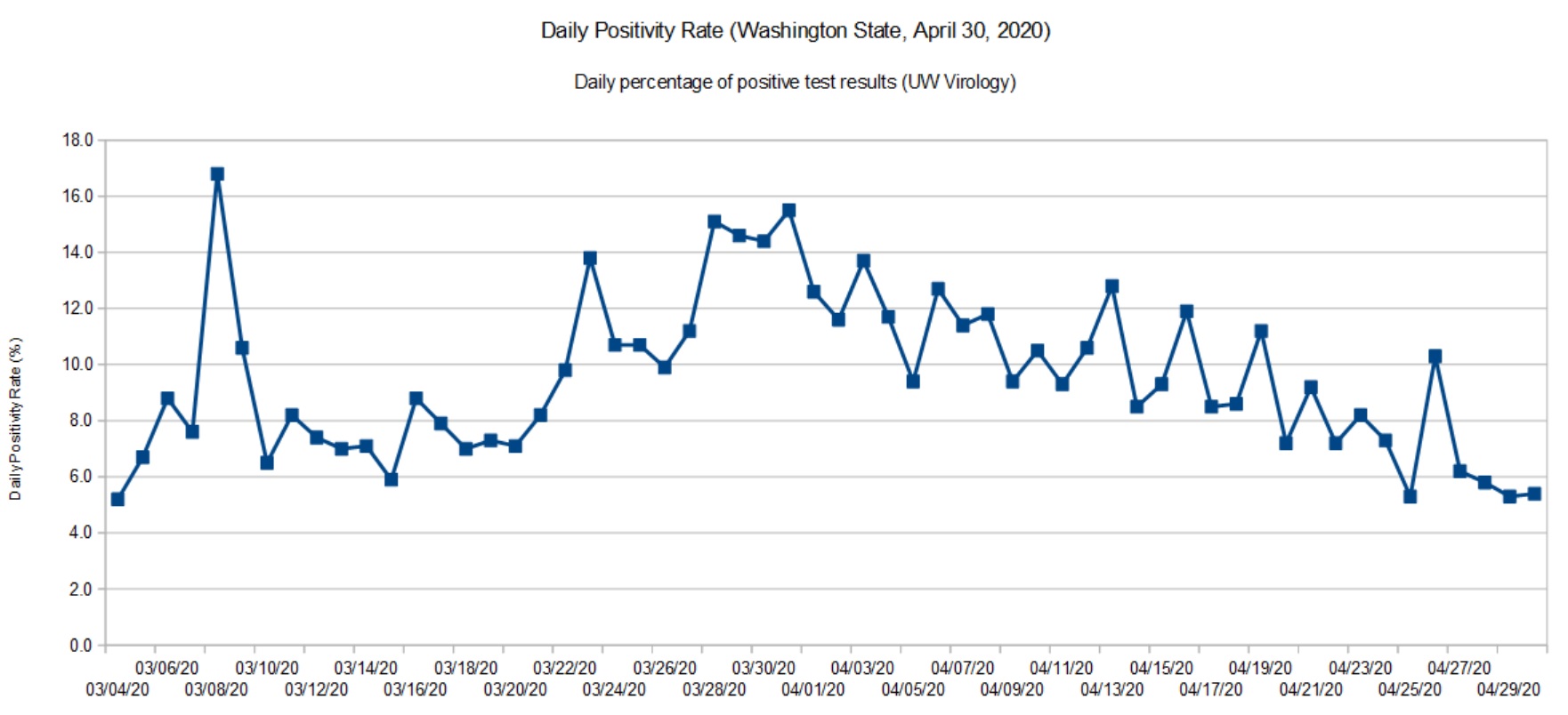
Washington State daily positivity rate (UW Virology, April 30, 2020)
The second graph is based on data for the University of Washington (UW) Virology Laboratory. The UW chart is up-to-date because they don’t have the same aggregation and reporting responsibility as DOH. For UW, it’s specimens in, and test results out. The UW results are sent to DOH where they are eventually folded in.
Both graphs show a steady decline. In terms of positivity rate, we’re back to where we were in mid-March. The peak occurred around March 28.
SARS-CoV-2 is still circulating in the community. I think Governor Inslee has made the right decision to go slow on “re-opening.”
The positivity rate is an imperfect indicator of the actual infection rate in the general population. Given the total number of confirmed cases (14,327) and assuming that ten times as many people are actually infected (143,000), that’s an overall infection rate of 2%. Normally, a disease doesn’t slow down until the infection rate is 50% to 60% (so-called herd immunity). Two percent is insignificant and SARS-CoV-2 could easily “burn” through the population if it is left unchecked.
Are we heading toward 1918, again?
The Centers for Disease Control and Prevention (CDC) site has an extensive section about the 1918 influenza pandemic in the United States. The pandemic was caused by an H1N1 virus. The disease was first identified in the United States during the spring of 1918, eventually killing 675,000 people in the U.S. The number of deaths worldwide is estimated at 50 million people.
Due to poor record keeping and other factors, a true accurate tally of infections and deaths is not possible. All figures are estimates.
If you’re at all familar with recent events in the United States, the 1918 pandemic timeline should make your hair stand on end.
March 1918: Outbreaks of the flu are first detected. This is the beginning of the first wave.
April 1918: Cases and deaths are reported by public health officials.
Summer 1918: The first wave crests and declines.
September 1918: The second wave emerges.
October 1918: 195,000 Americans are killed by the virus during October alone.
November 1918: The fatal second wave subsides. America celebrates World War I Armistice (parades, etc.) setting up a third wave of infection.
December 1919: A third wave begins.
April 1919: The third wave subsides.
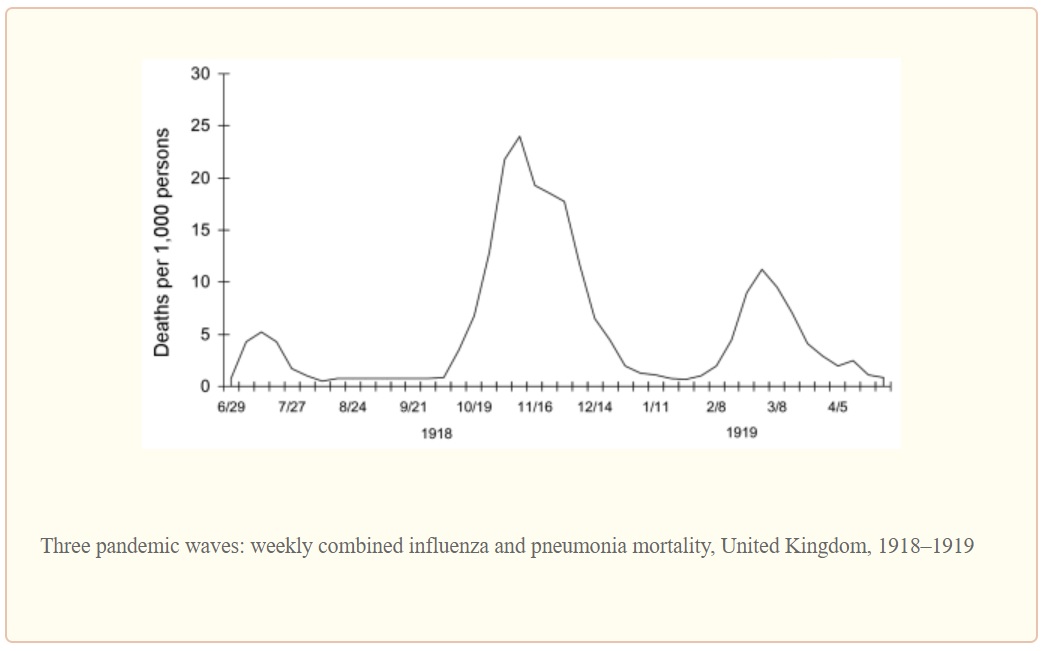
The second wave was the most deadly wave and was responsible for most of the losses in the U.S. The timing is eerily similar to the COVID-19 outbreak in the U.S.
The graph below illustrates the lethality of the three waves (as measured in the United Kingdom).
1918 Influenza: The Mother of All Pandemics, Taubenberger and Morens, January 2006
Barely two months into the COVID-19 pandemic, seventeen states are reopening partially and six states are lifting orders or reopening soon. [The New York Times, May 1, 2020] Some of the states have not satisfied the WhiteHouse/CDC gating criteria for reopening.
I fear that this is too soon to declare victory or to even imagine a return to a normal (pre-pandemic) state of affairs in one or two months. Dr. Anthony Fauci (NIH), Dr. Robert Redfield (CDC) and other health officials have warned about a second wave in Fall 2020. Be assured, SARS-CoV-2 will continue to circulate in the population during the summer months just like the 1918 H1N1 influenza virus. The American populace is just as vulnerable to an COVID-19 outbreak as it was in January 2020.
I genuinely hope and pray that we haven’t set outselves up for an extremely fatal second wave of COVID-19. Are we doomed to repeat history?
Stay the course and stay healthy — P.J. Drongowski